Mandibular Reconstruction using Fibula Graft
Head and Neck cancer accounts to 30% of all cancers diagnosed in India. Oral cancers are the most common among males in our country and fourth most common in females. In India 60-80% of them is present in advanced stage as compared to 40 percent in developed countries.
There is a primary need to understand the tumour location, shape, and size to realise an effective tumour removal followed by accurate reconstruction. The reconstruction is done by either using a customised implant manufactured in bio-inert material or by using patient’s own bone for grafting.
Here is one such case. A male patient of age 43 was diagnosed with cancer whose primary surgery of mandible tumour removal was already done. Due to deficient right mandible, there were difficulties in chewing, speech and for daily activities in public due to discomforting aesthetics.
Dr Raghuvir Solanki, Head and Neck Onco Consultant – Zydus Hospitals, approached our clinical engineers for a robust plan and precise reconstruction of the neo-mandible using the fibula bone of the patient.
We planned to Visualize, Plan, and then execute
Visualisation:
In order to visualise the mandibular anatomy and its neighbouring area, a high-resolution CT scan of adequate slice thickness and increment was used to 3D model the defect. Region of interest was well captured in the scan and replicated as 1:1 digital model for understanding the defect and pathology. Similarly, patient’s left fibula was modelled from the CT scan to harvest the required grafts. The idea is to provide self-explanatory model and help surgeon to make them visualize the information which usually remain hidden in conventional 2D CT images.
Planning:
Once the 3D modelling of the images (segmentation) was completed, a plan was to lay down the reconstruction of neo-mandible using fibula bone.
Key steps involved –
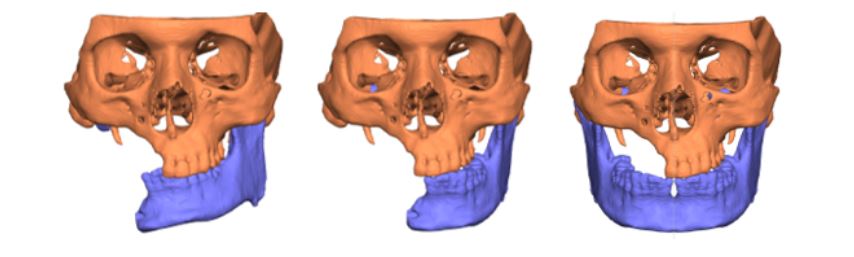
- Due to deficient region on the right, there was no contact to the right condyle, which resulted in improper occlusion.
- A proper occlusion was achieved by virtually simulating the correct occlusion state taking references from the mandibular/maxillary teeth and re-positioning the healthy left condyle in the fossa.
- Then the healthy left mandible was mirrored to achieve best clinical reference for reconstructing neo-mandible
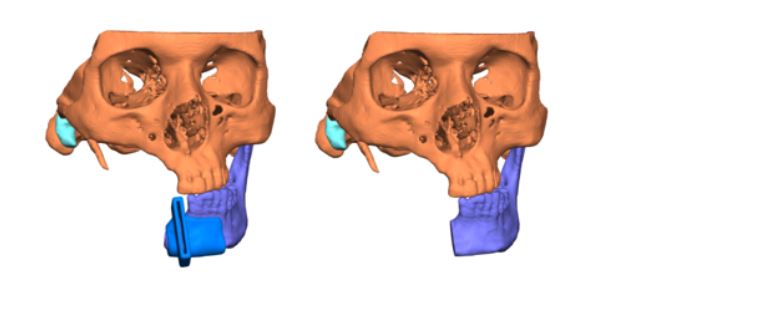
- Surgical guide was designed to resect the mandible for a perfect joint connection of new mandible to the healthy left mandible.
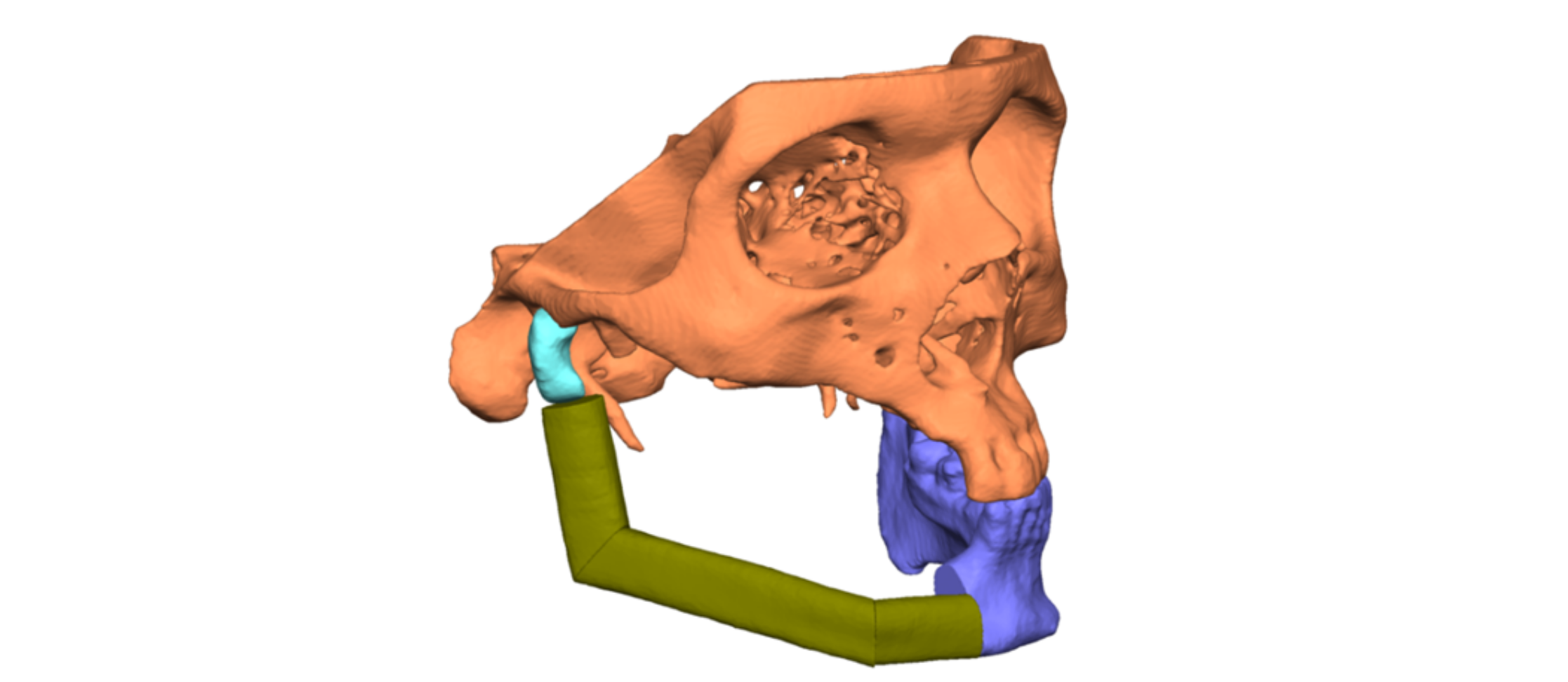
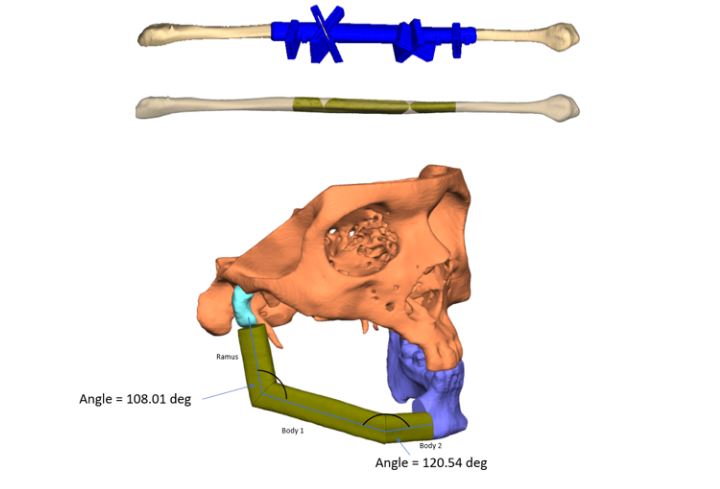
- Fibula bone was used to reconstruct the defect, following the reference of the mirrored side. This helped in getting the right segments of the fibula, placed at specific angles to form the new mandible for the patient. A surgical guide was designed to execute the exact same cuts intraoperatively.(As shown in below images)
3D Printing:
Once the surgical plan was approved and finalised, the plan was translated to physical models to analyse the outcome. Pre-op, intermediate and post-op models were printed. The patient-specific guides were 3d printed in biocompatible autoclavable material for realising the planned cuts intra-operatively on mandible and fibula bone.